Introduction
Transgender individuals are at a higher risk of psychiatric illness compared to cisgender individuals,1 a disparity that has been linked to the social stigma and discrimination to which they are subjected.2,3 Transgender individuals experience more adverse outcomes than lesbian, gay, and bisexual (LGB) individuals, owing in part to rejection and discrimination experienced even within the LGB community.4 Globally, transgender individuals face unemployment and encounter significant difficulties in accessing financial resources and securing employment.5 In India, the transgender community has similarly been found to struggle with access to limited economic opportunities,6 which are further diminishing as their traditional roles decline.7
The psychological distress experienced by transgender individuals in India manifests in the forms of anxiety, depression, and stress,8 with the prevalence of depression and anxiety reported to be high (61.25% and 63.75%, respectively).9 A study of 300 transwomen across four states of India found that 42.7% suffered from moderate to severe depression,10 while another study reported that 48% met the criteria for psychiatric disorders.11 Transgender individuals are also more likely to experience substance abuse, suicidal ideation, and suicide attempts.12 Indian transgender youth are particularly vulnerable to mental health difficulties as a consequence of poverty, abandonment, and social exclusion, compounded by inadequate policy support.13
Access to appropriate mental health services tailored to the needs of transgender individuals remains limited,14 and gaps in knowledge regarding how best to promote the wellbeing of this population persist.15 In India, research concerning transgender communities has largely focused on HIV; to the best of our knowledge, no interventions specifically targeting the promotion of mental health and wellbeing among transgender individuals have been conducted in the country. Such interventions have predominantly been carried out in high-income settings: a systematic review of mental health interventions for transgender and gender non-conforming individuals found that all 22 studies meeting the inclusion criteria were conducted in high-income countries.16
In this paper, we describe the findings of Manthan, a study that sought to promote the mental health and wellbeing of transgender individuals at high risk of anxiety and depression.
Methods
Study Area
The study was conducted among transgender individuals residing in the National Capital Region of Delhi (Delhi NCR).
Study Design, Objectives, and Hypothesis
This was a pre-post mixed-methods study with the following objectives:
-
To evaluate a trans peer support model for managing anxiety, depression, and suicidality/self-harm, and to explore its effects on anxiety, depression, suicide/self-harm, and the psychological wellbeing of transgender individuals.
-
To assess the acceptability of the trans peer support model and to identify facilitating and impeding factors.
The study hypothesised that participants would demonstrate improvement in Generalised Anxiety Disorder-7 (GAD-7),17 Patient Health Questionnaire-9 (PHQ-9),18 and World Health Organization Quality of Life (WHOQOL-BREF) scores at endline compared to baseline.19
Sample Size
A sample of 60 participants provided 90% power at a 5% level of significance, assuming a standard deviation of 10 points for paired differences and a 25% loss to follow-up, to detect a 5-point change in PHQ-9/GAD-7 scores, which is considered clinically significant.20
Inclusion Criteria: Participants at high risk of depression (PHQ-9 score ≥10 and/or a positive response [score ≥2] to the suicide risk item on the PHQ-9) and/or at high risk of anxiety (GAD-7 score ≥10).
Exclusion Criteria: Participants with severe physical ill-health, those who did not provide written informed consent, or those who were temporary residents of Delhi NCR.
Study Outcomes
Effectiveness Outcomes
Primary outcomes: Change in mean PHQ-9, GAD-7, and WHOQOL-BREF scores at 12 months from baseline.
Secondary outcomes: Change in mean Mental Health Knowledge, Attitudes, and Behaviour (KAB)21 and Barriers to Access to Care Evaluation – Treatment Stigma Subscale (BACE-TS)22 scores at 12 months from baseline.
Implementation Outcomes
Assessment of the feasibility and acceptability of the trans peer support model, and identification of barriers and facilitators.
Conceptual Framework Underpinning the Intervention
The Manthan intervention was guided by a theoretically informed logic model integrating principles from social support theory, behavioural activation, and trauma-informed care. The intervention was premised on the understanding that chronic exposure to stigma, discrimination, and social exclusion contributes to elevated anxiety, depression, and poor wellbeing among transgender individuals, and that peer-led psychosocial support can mitigate these effects through multiple interacting pathways. Psychoeducation components were designed to improve mental health literacy, symptom recognition, and self-efficacy; skills-based activities — including behavioural activation, mindfulness, grounding, and emotion regulation — were aimed at reducing psychological distress by strengthening coping and stress management capacities; and peer group processes were expected to enhance social connectedness, normalize lived experiences, and reduce internalized stigma related to mental health and help-seeking. These proximal mechanisms were hypothesized to collectively contribute to reductions in depression and anxiety, improvements in psychological wellbeing and quality of life, and enhanced knowledge, attitudes, and behaviours related to mental health care (Table 1).
Intervention and Implementation
The research team worked closely with a queer-affirmative therapist to develop the trans peer support model. The model was finalized following iterative discussions with a Trans Advisory Group (TAG) comprising ten members, including transgender individuals, a counsellor, and a clinical psychologist.
The intervention comprised 24 sessions delivered fortnightly to study participants in groups of approximately ten people. The sessions covered the concepts of sex, gender, and sexuality; mental health; self-care; building resilience; understanding emotions; managing stress, depression, and anxiety; preventing burnout; self-awareness; anger management; communication; handling peer pressure; suicide safety planning; and drafting personal mission and vision plans. The sessions incorporated elements of behavioural activation and included mindfulness activities, sensory grounding exercises, body scanning, deep breathing, and guided imagery.
Sessions were facilitated by transgender peers with the support of the research team. Peers were members of their respective groups, with two designated peers per group. The principal investigator (PI) trained the peers on the intervention modules across eight phases over the one-year intervention period.
Tools and Scales Used
The questionnaire comprised key instruments (Table S1) alongside questions relating to sociodemographic details. All instruments were translated into the local language prior to data collection.
Data Collection
Data were collected at three time points — baseline, midline, and endline. All data were collected electronically via REDCap (https://www.project-redcap.org/) by trained data collectors using seven-inch tablets. All data collectors, with the exception of one, were transgender individuals. There were no missing values.
Statistical Analysis
Quantitative data: Baseline characteristics were summarised using percentages for categorical variables, and means with standard deviations or medians with interquartile ranges for continuous variables. Paired differences in PHQ-9, GAD-7, WHOQOL-BREF, KAB, and BACE-TS scores were analysed using paired t-tests. Pre- and post-intervention suicide scores ≥2 were analysed using McNemar’s test. Dropout and withdrawal rates were analysed quantitatively to assess acceptability.
Qualitative data: Focus group discussions (FGDs) with study participants and in-depth interviews (IDIs) with relevant stakeholders were conducted to explore perceptions of the peer sessions, facilitating factors, barriers to participation, and reasons for discontinuation. FGD and IDI transcripts were translated into English and coded using an inductive approach.
Results
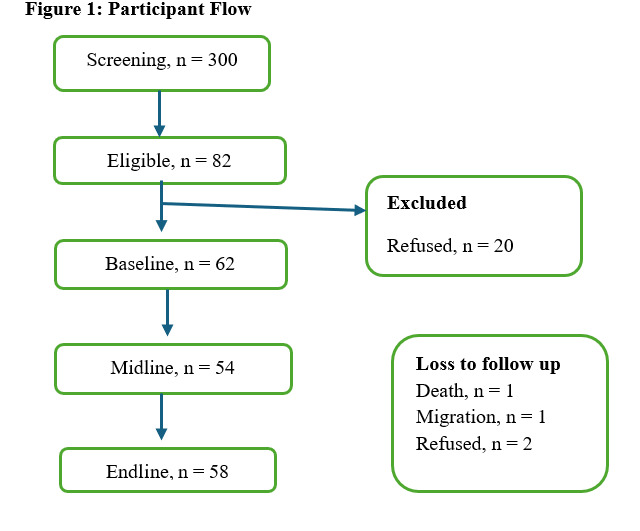
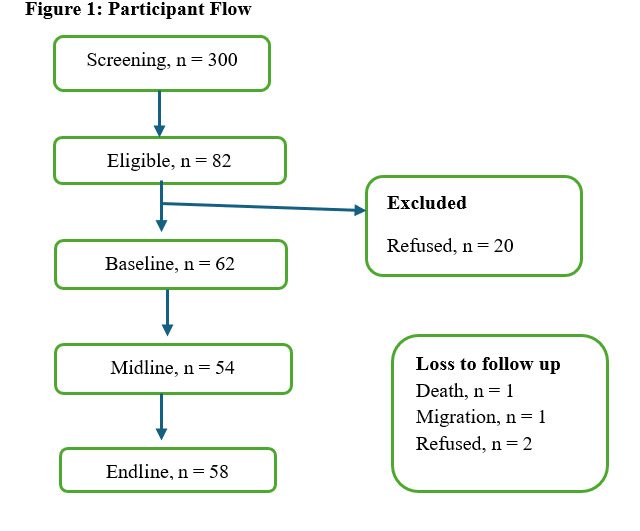
The intervention was implemented from September 2024 to August 2025. A total of 300 transgender individuals were screened, of whom 82 were identified as being at high risk of anxiety and/or depression, suicide risk, or self-harm. Of these 82, 20 declined to provide consent; baseline assessments were therefore administered to 62 individuals. A total of 54 (87.1%) and 58 (93.5%) participants were followed up at six months and 12 months, respectively (Figure 1).
Sociodemographic Profile
The majority of participants were transwomen (77.4%), with the remaining 22·6% identifying as transmen (Table 2).
The majority of study participants (50%) had either completed their graduate degree or were currently pursuing one, and a large proportion worked in the private sector (58.1%). A smaller number were engaged in sex work (9.7%) or supported themselves through begging (1.6%), and 17.7% were unemployed. With the exception of 27.4% of participants, all others were undergoing gender-affirming care to reflect their gender identity.
Effectiveness Outcomes
The mean PHQ-9 score demonstrated a statistically significant decline from baseline (13.1) through midline (Table S2 and Table S3) to endline (7.0) (Table 3). Similarly, the mean GAD-7 score declined significantly from 11.2 at baseline to 6.0 at endline. WHOQOL-BREF scores improved across all four domains from baseline to endline.
Knowledge, attitudes, and behaviours related to mental health improved from baseline to endline, and mean BACE-TS scores decreased over the same period.
Furthermore, a clinically significant 5-point change [20] in PHQ-9 scores was observed in 51.9% of participants at midline and in 60.3% at endline. A similarly clinically significant 5-point change in GAD-7 scores was observed in 50.0% of participants at midline and in 58·.6% at endline.
Implementation Outcomes
Mixed methods were employed to assess the acceptability of the trans peer support model. The outcomes measured were as follows:
i) Proportion of participants attending sessions: The median session attendance rate was 91.7% (95% CI = 70.8, 95.8).
ii) Reasons for discontinuation: Of the 62 transgender individuals recruited into the study, two did not attend a single session. Of the remaining 60, six dropped out after attending a few sessions (Table 4).
iii) Facilitators and barriers related to attendance:
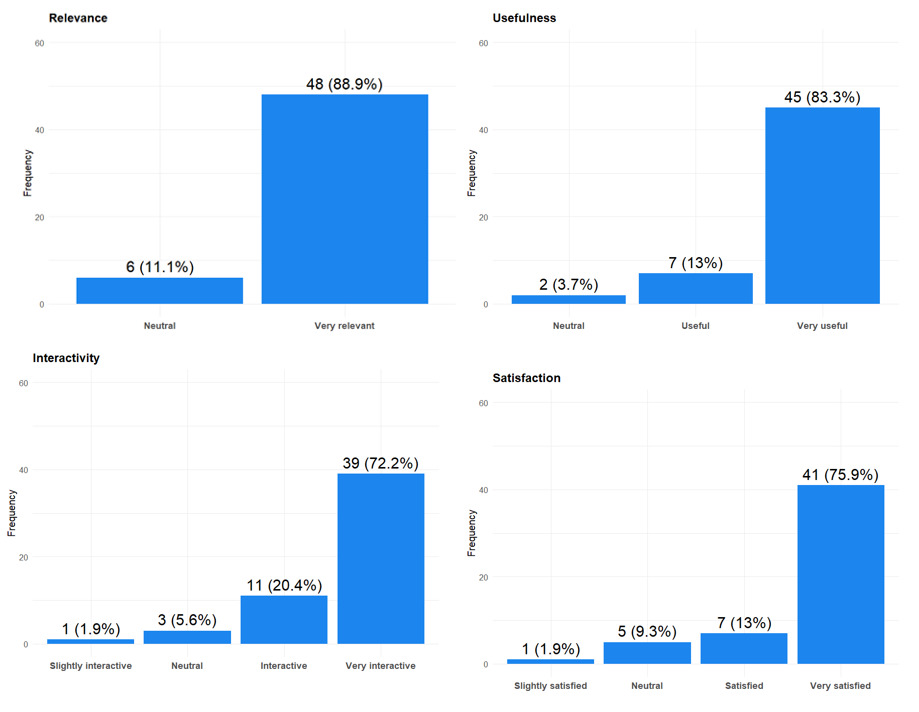
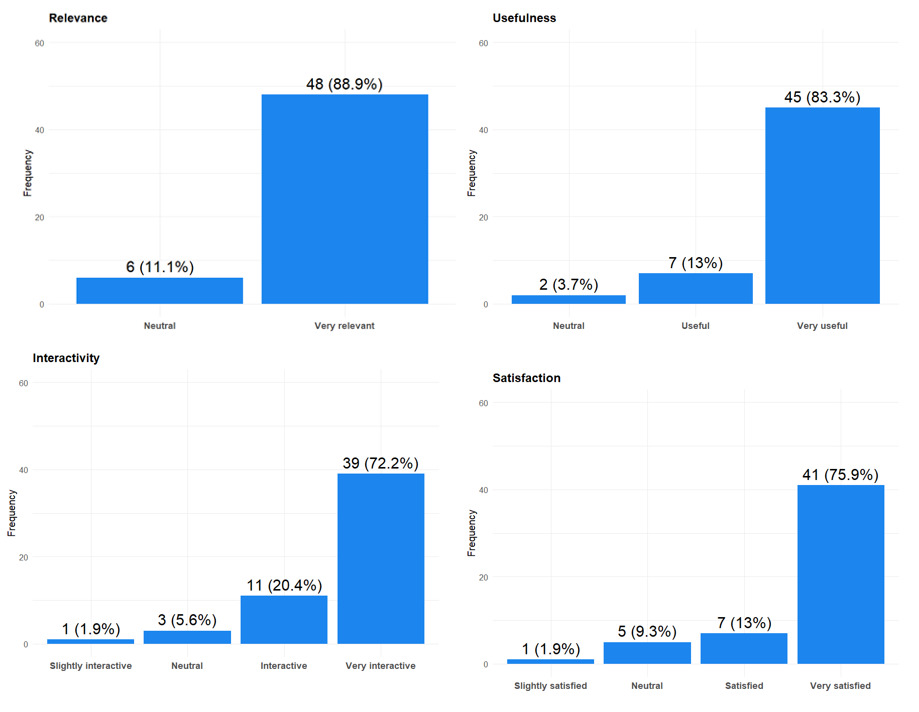
Facilitators: The majority of participants (88.9%) reported the sessions to be relevant, and 83.3% found them useful (Figure 2); 72.2% found them interactive, and 79.5% expressed a high level of satisfaction.
Discussions with participants revealed four main factors that facilitated attendance:
a. Session content: Session content was crafted with participants’ lives and struggles in mind, and was enriched with lived-experience case studies drawn from the queer-affirmative therapist’s practice, which participants found highly relatable. The sessions also incorporated games and activities that stimulated interest, encouraged creativity, and promoted self-reflection. As one participant noted:
“And then when we sit down to think; we recall so many things. Then we realized all that we had missed. I got quite a lot of help from that too, because all that we had left behind came back to us and we realized that those were the days that we had once lived and now we realize how much we missed. That also had a great effect. I learned a lot from that.” (IDI-5)
Participants also noted that the sessions helped them to acknowledge and recognise that they were experiencing mental health difficulties, and to identify ways of coping with them:
“And as long as you do not understand that there is a problem and identify it; you will not find a solution to your problems. So, I could identify for the first time; that, yes, I do have a mental health issue; which is troubling me and because of which I am facing anger issues. People often say that the wounds of the heart are laid open; but they do not apply any medicine on it. But Manthan has taught me that if there is a problem; then we should first identify it, after which we should discuss it, then find a solution [which may differ] from person to person.” (FGD-3)
b. Modality of delivery and the creation of a safe space: Sessions were delivered in peer groups, giving participants the opportunity to hear the experiences of others and to recognize that their peers were navigating similar struggles. This collective sharing of experiences fostered stronger interpersonal bonds:
“I was under the impression that all the other trans people are living very happy lives, and I am the only one on whom a mountain of sorrow had fallen. But no; I came to know that,…, that there are many whose situation is many times worse than mine… We got to see stories, where we found ourselves breaking apart. That was also a trigger for me.” (IDI-3)
This intimate sharing led participants to perceive their peer group as a safe space, where they experienced a sense of relief and calm:
“It always seemed as if we had come into another world, where there was peace of mind. When in reality, in our world, no one has any solace.” (IDI-6)
c. New learnings: Participants reported gaining meaningful knowledge about mental health through the sessions. They developed the ability to distinguish between anxiety, stress, depression, and burnout, and learned to recognise warning signs and triggers and to manage them effectively. Anger management was highlighted by almost all participants as being of particular importance. Moreover, many of the preconceptions that had initially made participants sceptical dissipated as the sessions progressed, and participants actively applied the coping strategies introduced during the peer group sessions:
“And if we know that the situation can get worse, we distance ourselves from it. We now go to positive places and meet positive people.” (FGD-2)
“I used to think that these mental health sessions are for mad people. I really used to think that it was meant for those who were mad. But then I got to know that it was for those who were overthinking and as a result not getting sleep at nights; this was to make that better.”(IDI-3)
d. Accessibility and flexibility: The sessions were made as accessible as possible and accommodated participants’ requirements to the greatest extent feasible. Session timings were flexible, and online sessions were offered to participants unable to attend in person. A modest travel bursary also contributed to participant retention.
The barriers that impeded participation were as follows:
a. For two participants, the group setting proved unsuitable. One identified as introverted and found the group format uncomfortable. The other was reluctant to share personal information within a group that included individuals with whom they had previously lived in a shelter home:
“Now, this is my personal life. I would not want my personal life to be known to others, would I?” (IDI-8)
b. One participant withdrew from the study as they were going through a particularly difficult period, experiencing severe depression and poor physical health. In this context, they felt that individual counselling would better meet their needs:
“It was a very dark phase. It felt that whatever I had achieved till now was going downhill…, I was so overwhelmed at that point that I needed proper counselling. The group sessions were, no doubt very well designed and well curated; but at that moment, I had reached my peak in depression. I was actually looking for counselling.” (IDI-2)
c. A further barrier was the time required for travel. Some participants lived at a considerable distance from the session venue and faced journey times of up to two hours, which resulted in them missing some sessions.
Discussion
The majority of research concerning transgender individuals in India is HIV-centric; the few studies that have focused on mental health have been descriptive in nature and have not tested interventions aimed at promoting mental health. Some HIV-focused programmes have included mental health support as one of several services offered to participants. For instance, the Pehchan programme aimed to strengthen community systems and provide HIV, health, legal, and social services to transgender communities across 18 Indian states.23 Its findings demonstrated significant increases in community-based demand for services, including psychological services (mental health service use increased to 33·0%, p<0.001) over the lifetime of the programme. Pehchan also underlined the importance of peer support networks in promoting service uptake. A study conducted in Lebanon (TransAction)24 sought to improve social cohesion, community connectedness, and the mental and sexual health of transgender women of mixed HIV status. TransAction comprised six distinct modules delivered by a trained transwoman once a week over a six-week period to 16 adult transgender women. The intervention was found to have high feasibility and acceptability, and participants reported valuing the peer group experience.
Mental health intervention studies involving transgender individuals have been conducted largely in high-income settings. A study conducted in the United States delivered a brief online intervention — a video about positive transgender identity — to transgender youth and found that depressive symptom scores among participants in the intervention arm were lower than those of control arm participants, who were shown a video containing general information about LGBTQ people.25 Another study by Clements et al. (2021),26 which aimed to increase wellbeing and resilience among transgender and non-binary participants by engaging them in focus groups and in the creation of videos of personal narratives highlighting positive identities, found increases in positive identity and wellbeing. A pilot study evaluated the feasibility and effectiveness of an eight-module affirmative cognitive behavioural coping skills group intervention among 30 sexual and gender minority youth in Canada, and found a statistically significant reduction in depression (p<0.001) and an increase in reflective coping over the study period.27 Text message-based delivery of psychoeducation and skills content — twice weekly over a six-week period — resulted in statistically significant reductions in anxiety (p=0.01) and depression (p<0.05) post-intervention, as well as an increase in social support among participants.28
The impact of peer support on people with mental illness has been demonstrated in high-income countries through both qualitative and quantitative studies; peer support has been associated with increased empowerment, hope, quality of life, self-esteem, and a greater sense of social inclusion, leading to increased care-seeking.29,30 Such interventions draw on the shared lived experiences of participants, which can reduce stigma and increase the acceptability of mental health services. Evidence for the positive effects of peer support from low- and middle-income countries (LMICs) remains more limited, though it is growing.31,32 In India, one project focused on building peer and family support groups led by individuals with lived experience of mental health conditions, with the aims of promoting human rights, empowerment, and recovery.33
Peer support and community safe spaces have also been found to be beneficial for other vulnerable populations that experience stigma, such as sex workers. Sex workers across Germany, Italy, Sweden, and the United Kingdom have reported that peer support was crucial to their mental wellbeing, as it was non-judgemental and non-stigmatising.34 Manthan presents findings from a peer support intervention designed to improve mental health outcomes for transgender individuals — a community that is vulnerable, marginalised, and subject to stigma and rejection. The results indicate that the intervention was effective: depression and anxiety decreased, and mental wellbeing improved. This is particularly significant given the substantial burden of mental illness faced by this community. Manthan highlights the importance of psychotherapeutic interventions and inclusive social environments for promoting mental health, and demonstrates that such interventions can be delivered by non-mental health professionals. The peer support model employed in Manthan reaffirms earlier research findings that social support — including in the form of peer support35 — plays a protective role in mental health.36,37 While Manthan did not specifically focus on building resilient coping, which has been linked to agency and self-acceptance,38 the intervention content did address assertive communication and self-acceptance, particularly in relation to the emotions experienced by participants.
While peer support interventions for transgender and gender diverse populations have largely been evaluated in high-income settings and are often brief, clinician-assisted, or embedded within HIV or biomedical programmes, Manthan extends this literature in several important ways. First, it is one of the few interventions conducted in a LMIC context that places mental health and wellbeing — rather than HIV prevention or treatment — at the core of the programme. Second, unlike many short-duration group or digital interventions, Manthan was delivered over a 12-month period, enabling sustained engagement, skill reinforcement, and relationship building among peers. Third, the intervention was designed and implemented through a community-engaged, peer-led model with extensive input from transgender individuals themselves, demonstrating the feasibility of delivering structured psychosocial support without sole reliance on specialist mental health professionals, who remain scarce in such settings. In doing so, Manthan contributes evidence for a scalable, low-cost, and culturally grounded peer support model that addresses the mental health needs of transgender individuals in resource-constrained settings. Taken together, Manthan demonstrates how a multicomponent, peer-delivered psychosocial intervention can be adapted and sustained within an LMIC context, building on global peer support models while addressing gaps in duration, scope, and community leadership that have remained underexplored in the existing literature.
Given the progressive legislation that India has adopted, a psychosocial intervention such as Manthan could be scaled up seamlessly within the country. Over the years, India has implemented a range of progressive administrative and legislative initiatives aimed at promoting the welfare of transgender and gender diverse people.39 The National Legal Services Authority vs Union of India (NALSA) judgement, hailed as a landmark Supreme Court ruling in 2014,40 upheld the right of transgender and gender diverse individuals to self-identification of their gender as a third gender. Subsequently, the Transgender Persons (Protection of Rights) Rules of 202041 prohibited discrimination against transgender individuals. The Ministry of Social Justice and Empowerment has taken active steps to promote their welfare, including the establishment of shelter homes (Garima Grehs) for transgender individuals. The Government of India has also designated dedicated outpatient days at selected public health facilities, which provide free treatment and investigations, particularly in relation to gender-affirming surgeries.41 Peer support models such as Manthan could be integrated into the services offered by these public health facilities and shelter homes, providing a composite package of interventions that addresses the mental health needs of transgender individuals.
Strengths and Limitations
The majority of interventions undertaken to address the mental health concerns of transgender individuals have been short-term in nature, ranging from a few weeks to a few months, which raises questions about their long-term effects. Manthan, by contrast, with its 12-month intervention period, provides more robust data on the long-term effects on clinically relevant mood and anxiety symptoms, with clear indications of beneficial changes in quality of life. While the multicomponent nature of the intervention limits the attribution of effects to individual components, it reflects real-world delivery conditions and aligns with community preferences for holistic, peer-led support.
However, the mean depression and anxiety scores of participants at endline remained at mild levels, suggesting that additional mental health support may be required for those who continued to show residual symptoms. Manthan had a relatively small sample size and employed a quasi-experimental design, which limits the generalizability of the findings. Given the modest sample size, two-time-point pre-post structure, and limited number of covariates, paired t-tests were considered the most appropriate analytical approach. Furthermore, Manthan was conducted in a single city, which further constrains the generalizability of the findings. Additionally, while effectiveness outcome data were collected by data collectors external to the intervention, the qualitative data informing the acceptability assessment were collected by the Manthan team itself, which may have introduced socially desirable responding. Future studies employing larger, multisite samples, a controlled or randomised design, additional follow-up time points, and mixed-effects models would enable more robust analyses capable of accounting for participant-level heterogeneity and potential confounders.
Conclusion
Manthan is one of the first studies in India to have tested an intervention aimed at promoting the mental health and wellbeing of transgender individuals. The results are promising, with reductions in anxiety and depression and improvements in the mental wellbeing of participants. Consistent improvements across mental health, quality of life, attitudes, and behaviours further support the value of extending such interventions to a broader segment of the community. A randomized controlled trial involving multiple study centres would provide more robust evidence and help inform mental health policy in India, with a specific focus on the mental health of transgender individuals. The programme also demonstrates strong translational potential beyond research settings. Manthan aligns with existing government programmes supporting the social integration of transgender individuals, and the inclusion of such low-cost yet effective interventions within initiatives such as the Garima Grehs could contribute substantially to improving the mental wellbeing of transgender individuals, particularly in resource-constrained settings.
Author Contributions
The study was conceptualized by SKY in discussion with all authors. Data analysis was conducted by AR. SKY drafted the original manuscript, which was reviewed and edited by MKB and NAK. PKM and VS provided critical inputs. All authors reviewed previous versions of the manuscript and approved the final version.
Role of the Funding Source
This research was funded by the Indian Council of Medical Research (ICMR) (Grant EMTR/SG-DL/2023/07-3). The funders had no role in study design, data collection, data analysis, interpretation of findings, or writing of the report.
Declaration of Interests
The study was funded by the Indian Council of Medical Research (ICMR) (Grant EMTR/SG-DL/2023/07-3). MKB is fully supported by the ICMR grant. NAK and SKY are fully or partially supported by the Adolescent Resilience-Building in Urban Slums: A Multifaceted Implementation Trial of Life Skills Education in India (ANUMATI 2.0), funded by the NHMRC (NHMRC/GACD Grant 2022355). PKM is partially supported through a DBT/Wellcome Trust India Alliance Senior Fellowship (IA/CPHS/21/1/505968) for a randomized controlled trial evaluating a technology-enabled platform for managing depression with or without behavioural activation in patients with cancer in India, and through ANUMATI 2.0. PKM is Co-Principal Investigator on ANUMATI 2.0 and on the India Alliance Clinical/Public Health Research Centre Grant (IA/TSG/20/1/600061) for the Scaling-up the Competency of Primary Care Workers to Manage Epilepsy by Task-Sharing (STOP-Epilepsy) study.
Ethics Declaration
All procedures involving human participants were conducted in accordance with the ethical standards of The George Institute for Global Health, New Delhi, India (Ref. No. 23/2023). The study was conducted in accordance with the principles of the 1964 Declaration of Helsinki and its subsequent amendments.
Acknowledgements
This study is the outcome of a deeply collaborative, community-engaged, and participatory research process, made possible through the generous contributions, guidance, and support of numerous individuals and organizations. We begin by expressing our sincere gratitude to the members of the TAG, whose insights, lived experiences, and critical feedback shaped every stage of this study — from conceptualization and design through to implementation and interpretation. Their sustained engagement ensured that the research remained grounded in community realities, ethically responsive, and attentive to the diverse needs and priorities of transgender persons. We extend our deepest appreciation to Srabasti Majumdar, a Kolkata-based queer-affirmative therapist, whose expert guidance and mentorship ensured that the intervention module was trauma-informed, inclusive, and community-affirming. We are also sincerely grateful to our collaborating organizations — Tweet Foundation, Basic Foundation, Satrangi Samaj Foundation, and Balvikas Dhara — for their invaluable support in community outreach, participant engagement, and on-ground implementation. Their longstanding grassroots work, the trust they have built within the community, and their continued collaboration were instrumental in enabling ethical and meaningful research engagement. Finally, we thank all peer leaders and study participants who generously shared their time, experiences, and perspectives. Their openness, trust, and contributions form the heart of this study, and we remain deeply grateful for their participation. This research would not have been possible without these collective efforts, and we extend our heartfelt thanks to all who were part of this journey.
Consent
Written informed consent was obtained from all study participants.
Data Sharing Statement
Relevant anonymised data, metadata, and the study protocol are available from the corresponding author and can be shared for research purposes upon request, subject to a data-sharing agreement, following publication of this paper.