1. Introduction
Schizophrenia is a chronic and severe psychiatric disorder, characterized by positive, negative and cognitive symptoms, although most patients respond to antipsychotic treatment, between 20% and 30% not response to pharmacological treatment.1
Electroconvulsive therapy (ECT) is a third-line treatment option; its indications include treatment resistance, catatonia, severe affective symptoms, suicide risk, and conditions such as refusal to oral medication.2
ECT can cause side effects; the most commonly reported are mild and temporary cognitive disturbances such as confusion, brief amnesia, headache, and muscle discomfort, usually self-limited.3 Tolerance is good and serious events such as cardiovascular complications are rare.4 There are reports of episodes of mania associated with ECT, most of these reports are in patients with bipolar disorder, it is infrequent and underreported in patients with a primary diagnosis of schizophrenia.5,6 ECT-induced mania is challenging to diagnose and treat because there are few reports in the literature to date.7
The present paper presents a clinical case of mania after ECT administration in a patient diagnosed with schizophrenia, an infrequent phenomenon that can lead to difficulties in the treatment of patients with severe psychotic conditions.
2. Case
A 27-year-old man with a history of harmful use of multiple substances since the age of 16, mainly alcohol, tobacco, volatile solvents, cocaine and cannabis. The specific pattern of consumption (frequency, quantity, and last consumption) is difficult to pin down due to the patient’s clinical, as well as the limited information provided by their support network. At the age of 18, he underwent a right nephrectomy secondary to open abdominal trauma from a sharp weapon, with no evidence of renal dysfunction documented so far. He lives with his father, who has alcohol addiction.
Psychotic symptoms began at age 16, characterized by persecutory and harm-related delusions, including the conviction that his neighbors were speaking ill of him, wanted to harm him, and had cameras installed inside his home to monitor him. He also reported that he could hear his neighbors through the walls, which was accompanied by homicidal ideation toward them. In addition, he presented with somatic and harm-related delusions, stating that medical staff intended to remove his kidney, as well as believing that he had undergone medical procedures without his consent and that “metal” had been inserted into his body.
In addition, other disturbances in thought content were documented, including phenomena of thought diffusion, insertion and reading, as he stated that others could access his thoughts, that they could communicate with him through telepathy, and that he himself could influence nature through body gestures.
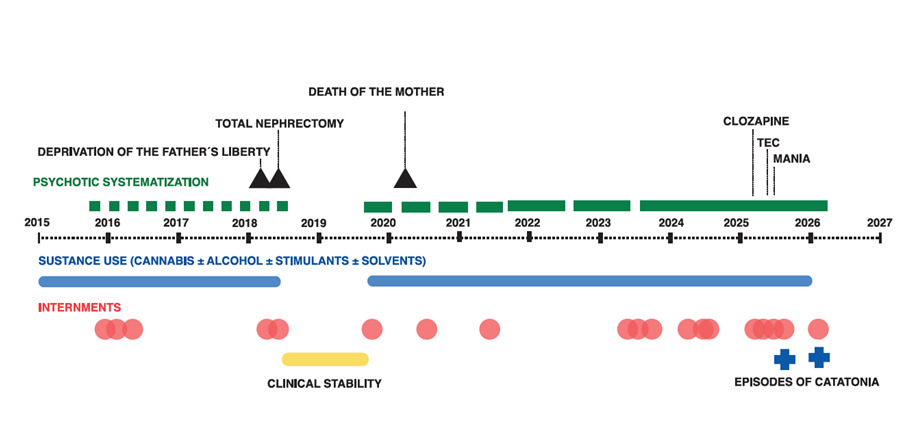
At age 20, he required his first psychiatric hospitalization due to the symptoms described above. Since then, his psychotic symptoms have persisted throughout multiple hospitalizations. He has been readmitted on several occasions due to poor adherence to pharmacological treatment, inadequate medical follow-up, and continued use of psychoactive substances. He has received various treatment regimens (including haloperidol, levomepromazine, flupenthixol, olanzapine, and clozapine), though the exact duration of these regimens is unknown due to limitations in adherence and the support network. He was also admitted to addiction rehabilitation centers for periods of approximately three months, during which cessation of psychoactive substance use was reported, but psychotic symptoms persisted. Based on the clinical course described, a diagnosis of schizophrenia was established. See Figure 1.
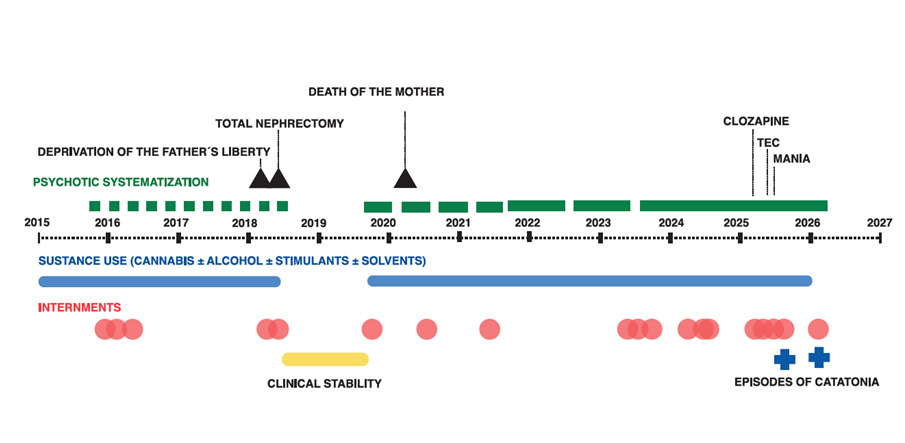
Figure 1 shows a trend toward progression of the clinical course, with psychotic episodes becoming longer in duration over time. Significant life events are identified, such as the father’s incarceration and the mother’s death—an event that coincides with ongoing psychotic symptoms. Consistently, no sustained affective episodes over time are documented that would suggest a primary mood disorder.
The most recent hospitalization was due to poor adherence to clozapine, which led to auditory hallucinations and aggression toward his neighbors. During the clinical evaluation, disorganized thinking was evident, manifested by incoherent speech, loose associations, difficulty maintaining a logical train of thought, and tangential responses. Treatment was initiated with olanzapine, a medication to which he had previously responded best; however, after 30 days at a dose of 20 mg/day, there was no improvement, and given the persistence of psychotic symptoms with targeted homicidal ideation, it was decided to initiate ECT.
The ECT protocol includes laboratory tests (complete blood count, blood chemistry), an electrocardiogram, an electroencephalogram, a brain CT scan, and a plain chest X-ray to assess cardiovascular and general physical risk.
ECT was administered via bifrontotemporal placement using a MECTA Spectrum 5000Q electroconvulsive therapy machine. In accordance with the characteristics of the available equipment, a method of individual estimation of the seizure threshold was employed using ascending titration of the charge. See Table 1. The same anesthetic regimen was used in all sessions, consistent of induction with propofol at a dose of 140 mg and neuromuscular blockade with succinylcholine at a dose of 70 mg. Continuous monitoring of hemodynamic and respiratory variables was performed during the procedure.
Seizure quality was assessed according to the CASBAS criteria (8,9), which include epileptiform discharges lasting longer than 20 seconds, with slow-wave activity exceeding 150 mV; a heart rate exceeding 110 bpm; interhemispheric symmetry greater than 85%; and the presence of postictal suppression.
The first three ECT sessions were administered on consecutive days, while the fourth was administered three days later. Beginning with the third session, a gradual and progressive onset of manic symptoms were documented, consistent on expansive mood, increased psychomotor activity, logorrhea, decreased need for sleep, impulsive behavior, and an attempt to leave the hospital. The Young Mania Scale score was 39 points. Given the severity of the clinical presentation, the patient left the hospital without authorization, which prevented the complete documentation of the course and resolution of the manic symptoms.
One month later, the patient was readmitted with a clinical presentation characterized by catatonia and homicidal ideation, without symptoms of mania. Treatment was initiated with 100 mg IM of extended-release paliperidone, 750 mg/day of valproic acid sodium, and 3 mg/day of lorazepam, resulting in clinical improvement, with the Brief Psychiatric Rating Scale score dropping from 38 points at admission to 4 points at discharge.
3. Discussion
The onset of mania after ECT is a rare complication that is scarcely described in the literature. Most of the reports correspond to isolated cases, without sufficient data to establish frecuency or evolution. In a case described in India, a patient with catatonic schizophrenia developed mania after the start of ECT treatment, in whom it was decided to add an antipsychotic and continue the therapeutic cycle, although follow-up was not reported.7 Mania induced by TEC has been described more frequently in patients with affective disorders, particularly in those with bipolar disorder treated for depressive episodes.8,9
It is not a distinct clinical phenotype, but a typical manic episode whose characteristic feature is its onset immediately after one or more ECT sessions. Various reports indicate that the symptoms correspond to the classic manic episode, which appear 1–2 days after ECT10,11; these case reports agree that the immediate temporality after ECT is rather than an atypical symptomatic pattern.
However, the onset of a manic episode following ECT requires a careful reconsideration of the differential diagnosis, especially in patients with a complex psychiatric history. This context highlights the need to consider alternative diagnoses such as substance-induced mood disorder or the possible presence of previously unrecognized bipolar or schizoaffective disorder. According to the DSM-5-TR, when manic symptoms meet syndromic criteria and persist beyond the immediate effect of the procedure, the possibility of a manic episode in the context of bipolar I disorder should be considered.12 In this regard, a thorough medical history, an examination of family and personal history of affective symptoms, as well as close longitudinal follow-up, are essential to clarify the diagnostic course and rule out schizoaffective or bipolar disorder.13
Although temporal association alone does not establish definitive causality, in this case, the absence of identifiable alternative triggers and the close temporal proximity between the administration of the treatment and the onset of symptoms suggest that the ECT was the triggering factor. To support this interpretation, the Naranjo scale14 was applied to assess causality in adverse reactions, yielding a score of 5, which corresponds to a probable association between the ECT and the manic episode.
A neurobiological perspective suggests that ECT may be associated with transient changes in dopaminergic circuits and in the modulation of D1 receptors in limbic/hippocampal regions, which could contribute to the onset of affective symptoms.15
Regarding treatment, there is no consensus on the course of action to follow; one review identifies four potential treatment options: (1) discontinuation of ECT, (2) discontinuation of ECT and initiation of pharmacological treatment, (3) continuation of ECT, and (4) continuation of ECT in combination with lithium.16 A favorable response to the use of mood stabilizers has also been documented, regardless of whether ECT is discontinued or continued.10
4. Conclusion
The occurrence of post-ECT mania in patients with resistant schizophrenia, although rare and poorly documented, is clinically relevant because it can modify the clinical course of the disease. This case emphasizes the need for systematic and close follow-up during early ECT sessions.
Contribution of each of the authors
All the authors presented contributed at all stages in the conception of this case report.
Ethical aspects
This work adheres to the ethical principles of the Declaration of Helsinki and the institutional standards for data protection and confidentiality of patient information. In accordance with Mexican legislation, informed consent was requested from the patient and responsible family member.